Clinical Skills
Mastering abdominal inspection, palpation, and percussion is essential for accurate GI diagnosis. This comprehensive guide covers systematic examination techniques and the interpretation of abdominal findings in clinical practice.
👁️ ABDOMEN INSPECTION
Visual Assessment Principles
Contour Assessment:
🎯 Normal, Distended, or Scaphoid?
- Scaphoid: Starvation, malignancy (esophagus/stomach cancer)
- Distended: Think 7 Fs
🎯 The 7 Fs of Distension
- Fat
- Fluid (ascites)
- Flatus (gas)
- Feces
- Fetus (pregnancy)
- Fibroid (uterine tumor)
- Full bladder
Movement & Vascular Patterns:
🎯 Abdominal Movement
- Normal: Gentle rise with inspiration, fall with expiration
- Absent/reduced: Generalized peritonitis ("still, silent abdomen")
- Visible peristalsis: Gastric outlet obstruction
🎯 Vein Assessment
- IVC obstruction: Flow upwards
- Portal hypertension: Caput medusae (distended veins around umbilicus)
📏 THE 9 ABDOMINAL REGIONS
Anatomical Landmark System
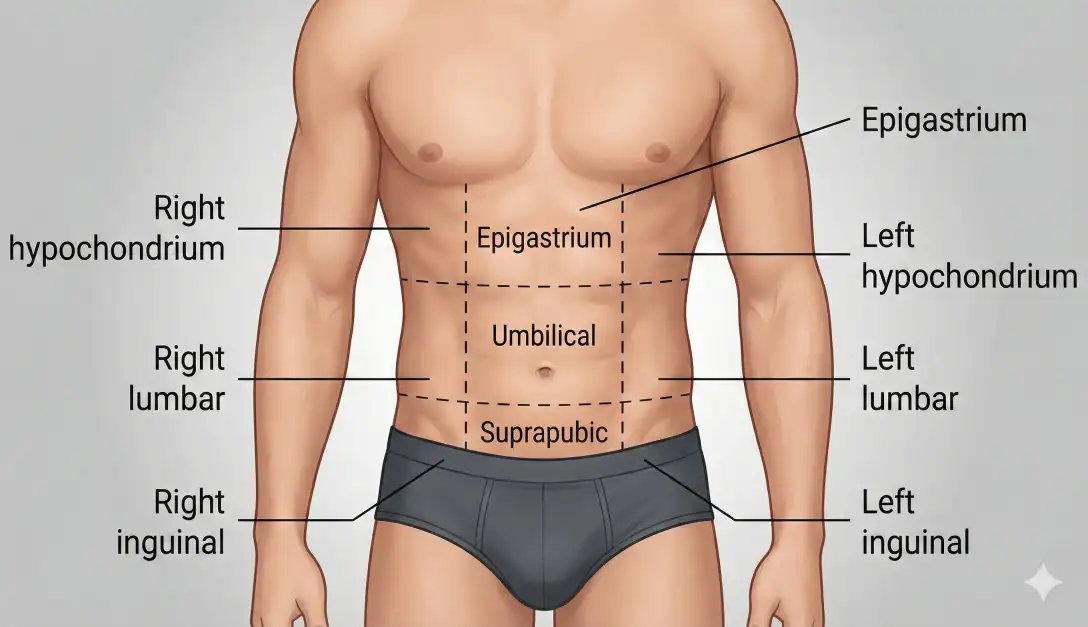
Regional Division:
🎯 Upper Abdomen
- Right hypochondrium (RH)
- Epigastrium (E)
- Left hypochondrium (LH)
🎯 Middle Abdomen
- Right lumbar (RL)
- Umbilical (UR)
- Left lumbar (LL)
🎯 Lower Abdomen
- Right iliac fossa (RI)
- Suprapubic/Hypogastrium (H)
- Left iliac fossa (LI)
✋ PALPATION: Light Then Deep
Palpation Techniques
Setup & Positioning:
🎯 Examiner Position
- On patient's right side
- Use pads of fingertips, not tips
- Raise bed or kneel if needed
- Watch patient's face for tenderness
Palpation Sequence:
🎯 Superficial Palpation
- Purpose: Detect tenderness, note masses, assess guarding
- Technique: Gentle, systematic, cover whole abdomen
- If tender area found: Palpate that area LAST in deep palpation
🎯 Deep Palpation
- Purpose: Characterize masses, palpate organs
- For any mass, note: Location, size, consistency, tenderness, surface, edge
- Always listen for bruit!
🫀 LIVER PALPATION
Liver Examination Techniques
Palpation Technique:
🎯 Method
- Start in right iliac fossa (RIF)
- Use pads of fingertips
- Work upward with each breath
- Ask patient to breathe deeply
🎯 Documentation
- Record enlargement: cm below costal margin in mid-clavicular line
- Don't use "finger breadths"—inaccurate
Liver Characteristics & Pathologies:
🎯 Right Heart Failure
- Enlarged, soft, tender
- Hepatojugular reflex: Press liver → JVP rises
🎯 Metastases
- Gross enlargement
- May elevate right diaphragm
🎯 Hepatocellular Carcinoma
- Enlarged, firm, tender + bruit
🟢 GALLBLADDER ASSESSMENT
Gallbladder Signs
Key Clinical Signs:
🎯 Courvoisier's Law
- "If jaundice + palpable gallbladder → unlikely to be gallstone in common bile duct"
- Gallstones cause chronic inflammation → fibrotic, small gallbladder
🎯 Murphy's Sign
- Press right hypochondrium, patient takes deep breath
- Sudden catch of breath when gallbladder touches fingers = cholecystitis
🎯 Boas' Sign
- Hyperesthesia (an abnormal increase in sensitivity to sensory stimuli, such as touch or pain, making normal sensations feel more intense or even painful) over T9-11 posteriorly on right indicates cholecystitis
🩸 SPLEEN PALPATION
Spleen Examination
Palpation Technique:
🎯 Method
- Start in RIF
- Work diagonally upward to left costal margin
- Left hand in patient's left loin to lift spleen forward
- Feel for notch(a small indentation) on medial border (pathognomonic!: Indicates splenomegaly)
🎯 Size Classification
- 1-2 cm below costal margin: Tip enlargement
- 3-7 cm: Moderate enlargement
- >7 cm: Massive enlargement
Causes of Splenomegaly:
🎯 Massive (>7 cm)
- CML (Chronic Myeloid Leukemia), myelofibrosis, hyperreactive malarial splenomegaly
- Leishmaniasis, Gaucher's syndrome
🎯 Moderate (3-7 cm)
- Infection: TB, malaria, endocarditis, EBV
- Portal hypertension (cirrhosis)
- Hematological: Hemolytic anemia, leukemia, lymphoma
🫘 KIDNEYS PALPATION
Renal Examination
Bimanual Technique:
🎯 Right Kidney
- Left hand posterior (right renal angle)
- Right hand on right flank
- Hands parallel, fingers pointing to umbilicus
- Roll kidney between hands
🎯 Left Kidney
- Left hand posterior (left renal angle)
- Right hand on left flank
- Hands parallel but opposite direction
- Roll kidney between hands
How to differentiate Spleen Mass from Left Kidney Mass:
🎯 Spleen
- Can you feel the top edge? No (ducks under ribs)
- Palpable notch? Yes (medial border)
- Bimanually palpable? No
- Percussion? Dull
🎯 Kidney
- Can you feel the top edge? Yes
- Palpable notch? No (Kidneys has no notch)
- Bimanually palpable? Yes
- Percussion? Tympanitic (Air filled bowel in front)
📍 OTHER ABDOMINAL MASSES
Mass Localization & Diagnosis
Common Mass Locations:
🎯 Epigastric Mass
- Advanced gastric carcinoma: Hard, irregular, middle-aged/elderly
- Pancreatic cancer: May be palpable in epigastrium
🎯 Midline Pulsating Swelling
- Aortic aneurysm: Especially in arteriopaths
- Lateral expansion = diagnostic (not just forward pulsation)
- Listen for bruit
Regional Mass Differential:
🎯 Right Iliac Fossa Masses
- Young adult: Appendicular mass/abscess
- Chronic symptoms: TB, Crohn's disease
- Elderly: Cecal carcinoma
- Painless + lymphadenopathy: Lymphoma
🎯 Left Iliac Fossa Masses
- Diverticular disease/mass
- Feces in loaded colon
- Colon carcinoma
- Crohn's, lymphoma
📋 Summary Checklist for Exams
High-Yield Exam Points
Key Abdominal Exam Pearls:
- 7 Fs for abdominal distension
- Courvoisier's law: Jaundice + palpable gallbladder ≠ gallstones
- Murphy's sign = cholecystitis
- Palpable spleen notch is pathognomonic
- Both kidneys palpable = polycystic kidney disease
- Troisier's sign: Palpable left supraclavicular node in gastric cancer
- Always listen for bruits over masses