Clinical Skills
Part 2 focuses on systematic pulse assessment, precordial examination, and cardiac auscultation. Mastering these skills enables accurate detection of valvular disorders, heart failure, and structural cardiac abnormalities.
💓 The Pulse: Five Essential Assessments
Radial Pulse Examination
1. Rate Assessment:
🎯 Measurement Technique
- Count for 60 seconds (gold standard)
- Experienced: 15 seconds × 4
- Location: Lateral wrist above flexor retinaculum
🎯 Classification
- Bradycardia: <60 bpm
- Normal: 60-100 bpm
- Tachycardia: >100 bpm
2. Rhythm Analysis:
🎯 Regular Rhythm
- Consistent interval pattern
- Normal sinus rhythm
🎯 Regularly Irregular
- Patterned irregularity
- Ectopic beats in predictable sequence
🎯 Irregularly Irregular
- Chaotic, patternless rhythm
- Atrial fibrillation characteristic
- Pulse deficit: Apex rate > radial pulse
3. Volume Assessment:
🎯 Weak/Thready Pulse
- Shock states
- Hypovolemia
- Reduced stroke volume
🎯 Bounding Pulse
- Hyperdynamic circulation
- Fever, thyrotoxicosis, pregnancy
- Increased stroke volume
4. Pulse Character (Waveform):
🎯 Normal Pulse
- Quick upstroke
- Brief plateau phase
- Downstroke with dicrotic notch
🎯 Plateau Pulse
- Slow-rising character
- Cause: Aortic stenosis
- Obstructed ventricular outflow
🎯 Collapsing Pulse
- Rapid upstroke, steep downstroke
- Wide pulse pressure
- Test: Raise arm, palm on forearm
- Causes: Aortic regurgitation, ASD, VSD, hyperdynamic states
🎯 Pulsus Alternans
- Alternating strong/weak beats
- Significance: Left ventricular failure
🎯 Pulsus Bisferiens
- Double-peaked pulse
- Cause: Combined aortic stenosis & regurgitation
🎯 Pulsus Paradoxus
- Weaker pulse on inspiration
- (Normally stronger on inspiration)
- Causes: Asthma, LV failure, cardiac tamponade, constrictive pericarditis
5. Arterial Wall Assessment:
- Roll radial artery against radius bone
- Normal: No palpable structure
- Abnormal: Rubbery tube sensation indicates arteriosclerosis
🦵 Peripheral Pulse Assessment
Comprehensive Vascular Examination
Major Pulse Locations:
🎯 Upper Body
- Temporal: Anterior to ear
- Carotid: Between larynx and SCM
- Brachial: Medial antecubital fossa
🎯 Lower Body
- Femoral: Mid-inguinal point (ASIS to pubic symphysis)
- Popliteal: Posterior knee (flexed position)
- Posterior Tibial: Behind medial malleolus
- Dorsalis Pedis: Foot dorsum between medial malleolus and 1st metatarsal
Clinical Pearl: Delayed/weak femoral pulse in young patients suggests coarctation of the aorta—a critical finding requiring urgent evaluation.
🎯 Precordial Examination
Cardiac Palpation & Inspection
Inspection Elements:
- Visible precordial pulsations
- Surgical scars (indicate previous procedures)
- Chest wall deformities (pectus excavatum/carinatum)
- Asymmetrical chest movement
Palpation Findings:
🎯 Thrill Detection
- Palpable murmur sensation
- "Cat purring" quality
- Indicates turbulent blood flow
🎯 Apex Beat Location
- Most inferior/lateral palpable cardiac impulse
- Finger lifted perpendicular to chest wall
Apex Beat Localization:
🎯 Normal Position
- 5th intercostal space
- Mid-clavicular line
🎯 Finding Technique
- Locate angle of Louis (sternal angle)
- Identify 2nd intercostal space below
- Count down to 5th space
- Note relationship to mid-clavicular line
Displaced Apex Beat Causes:
🎯 Mediastinal Shift
- Toward pathology: Lung collapse
- Away from pathology: Pleural effusion/pneumothorax
- Confirm with: Tracheal position assessment
🎯 Left Ventricular Hypertrophy
- Displaced down and laterally
- Sustained, forceful character
🎯 Right Ventricular Hypertrophy
- Left parasternal heave
- Hand lifted off left sternal border
- Systolic lift sensation
👂 Cardiac Auscultation
Heart Sound Assessment
Stethoscope Selection:
🎯 Bell
- Low-frequency sounds
- Light skin contact
- Best for: Apex (S3, S4, mitral stenosis)
🎯 Diaphragm
- High-frequency sounds
- Firm skin pressure
- Best for: Base (S1, S2, murmurs)
Heart Sounds Identification:
🎯 S1 (First Heart Sound)
- Timing: Systole onset
- Cause: Mitral/tricuspid valve closure
- Correlate: Coincides with carotid pulse
- Loud in: Mitral stenosis
🎯 S2 (Second Heart Sound)
- Timing: Systole end
- Cause: Aortic/pulmonary valve closure
- Split: Physiological inspiration (A2 then P2)
🎯 S3 (Third Heart Sound)
- Timing: Early diastole
- Cause: Rapid ventricular filling
- Normal: Children/young adults
- Pathological: Heart failure, constrictive pericarditis
🎯 S4 (Fourth Heart Sound)
- Timing: Late diastole
- Cause: Atrial contraction against stiff ventricle
- Significance: Always pathological
- Indicates: Heart failure, ventricular hypertrophy
Classic Auscultation Areas:
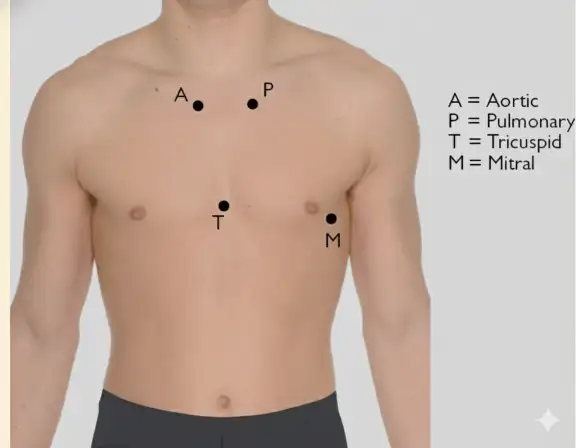
🎯 Mitral Area
- 5th intercostal space, mid-clavicular line
- Left ventricular sounds
🎯 Tricuspid Area
- 4th intercostal space, left sternal border
- Right ventricular sounds
🎯 Aortic Area
- 2nd intercostal space, right sternal border
- Aortic valve sounds
🎯 Pulmonary Area
- 2nd intercostal space, left sternal border
- Pulmonary valve sounds
Examination Tip: After assessing the four classic areas, complete your auscultation by listening systematically across the entire precordium to detect radiation of murmurs and additional findings.